, Erdem Yalçinkaya 1
, Huseyin Arikan 1
, Umut Sabri Kasapoglu 1
, Semiha Emel Eryuksel 1
, Sait Karakurt 1
, Erdem Yalçinkaya 1
, Huseyin Arikan 1
, Umut Sabri Kasapoglu 1
, Semiha Emel Eryuksel 1
, Sait Karakurt 1
Abstract
Aim: To investigate the association between ultrasound-derived rectus femoris and paraster-
nal intercostal muscle thickness and weaning outcomes in mechanically ventilated, critically ill patients, as well as their relationship with post-extubation non-invasive mechanical ventilation requirements and 28-day mortality.
Study Design: This prospective observational study included 69 mechanically ventilated adult patients undergoing spontaneous breathing trials in a medical intensive care unit. Demographic characteristics, clinical severity scores (modified Nutrition Risk in the Critically Ill [modified NUTRIC] score, Acute Physiology and Chronic Health Evaluation II [APACHE II], Sequential Organ Failure Assessment [SOFA], and Clinical Frailty Scale [CFS]), and ultrasonographic measurements of rectus femoris and parasternal intercostal muscle thickness were obtained at the 30th minute of the spontaneous breathing trial. Patients were classified into weaning success or failure groups based on the absence or presence of reintubation or death within seven days after extubation.
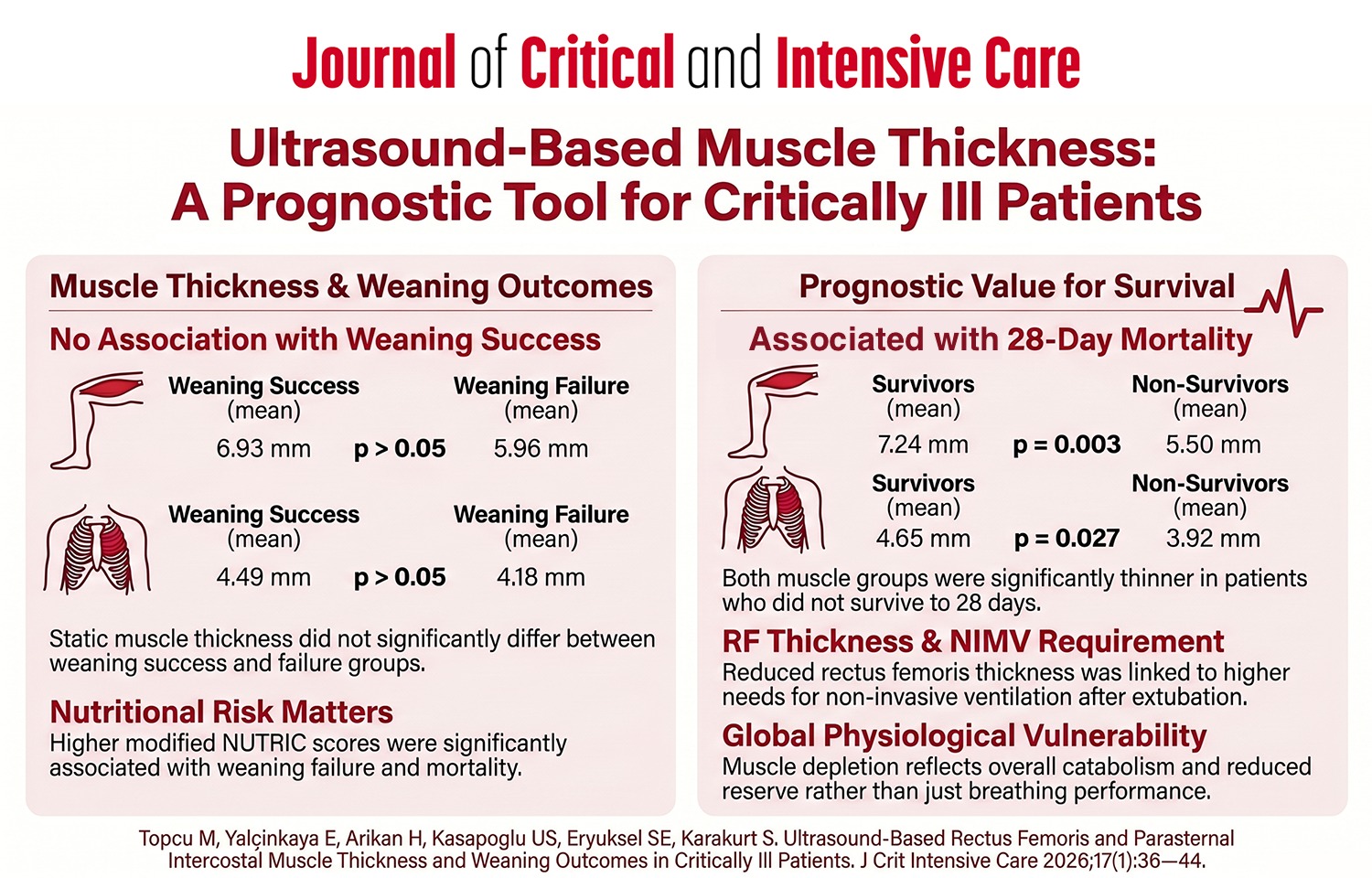
Results: The mean rectus femoris thickness was 6.93±2.31 mm in the weaning success group and 5.96±2.41 mm in the weaning failure group (p>0.05). Parasternal intercostal muscle thickness was 4.49±1.25 mm and 4.18±1.48 mm in the respective groups (p>0.05). Muscle thickness was not associated with weaning success; however, both rectus femoris and parasternal intercostal muscle thicknesses were significantly lower in non-survivors compared with survivors at 28 days. Reduced rectus femoris thickness was also associated with an increased requirement for post-extubation non-invasive mechanical ventilation. In addition, higher modified NUTRIC scores were associated with both weaning failure and 28-day mortality.
Conclusions: Ultrasound-based muscle thickness alone was not associated with weaning success; however, reduced rectus femoris and parasternal intercostal muscle thickness were associated with 28-day mortality and an increased requirement for post-extubation non-invasive mechanical ventilation. These findings suggest that ultrasound-based muscle assessment may provide useful prognostic insights for risk stratification in critically ill patients. Further multicenter studies are needed to validate standardized cut-off values and enhance clinical applicability.
Graphical Abstract